
The biological (medical) model
The medical (biological) model is the dominant view of mental disorder in Western society. The basic idea is that mental disorders are rooted in physical problems and that they require physical treatments to alleviate them.
To make sense of this we must bear in mind that psychiatrists are trained as medical doctors first. All medical doctors, from General Practitioners to anaesthetists and gynaecologists have been trained to treat physical disorders with physical interventions such as medications and surgery. Psychiatrists come from the same basic perspective and psychiatry itself has developed from that same, physical root.
So, according to the biological (medical) model of mental disorder all psychiatric problems are caused by physical imbalances or abnormalities. That’s why psychological problems get physiological treatments such as medications (chemicals used to change physical processes) or even surgery.
It is important to say that most psychiatrists in practice today see the medical model as only a partial explanation for mental disorder. Very few would stick rigidly to the idea that chemistry is everything but none the less this is a very powerful idea and it has a massive impact on mental health care today. In fact the development and supply of psychiatric medications based upon just this idea is a hugely profitable and influential worldwide industry in itself.
This is the opposite of the popular view that there is a difference between the ‘mind’ and the body. Many people, if asked, will insist that mental life is very different from physical life. However these people often do not think through their objections to the basic idea of the medical model.
Most people accept that hallucinogenic drugs like magic mushrooms and LSD affect perception. Drugs such as cannabis and ecstasy affect mood and substances like amphetamine (speed) can cause psychological problems such as paranoia as well as major emotional problems around anger and anxiety. These are psychological problems caused by physical (chemical) changes. If we accept that these things happen we must also accept that other types of physical changes cause psychological and emotional difficulties. They’re two sides of the same coin.
I’m always intrigued when people who use substances like cannabis, ecstasy or amphetamine tell me that their drug of choice doesn’t affect them psychologically. Clearly this cannot be the case or why on earth would they bother taking them? The fact is that people take recreational substances precisely because they affect mental and emotional life.
The medical model tells us that the fabled ‘mind:body’ split does not exist. Both are part of the same, single system. That is why physical interventions are used to make psychological and emotional changes. That is the essence of the biomedical model of mental disorder.
After all – if the problem wasn’t assumed to be caused by dodgy chemistry then what would be the point of giving chemicals in the form of medications to ‘fix’ it?
The social model
Many people argue that the social model is the opposite of the traditional medical model. Whereas the medical model places the cause of problems in affected person (the biologically ‘ill’ or physically ‘disabled’ individual) the social model is interested in the way that society at large reacts to people. It places responsibility for people’s problems as much in the lap of society as it does in the lap of the person themselves.
This does not mean that social perspectives deny the effects of physical or chemical processes such as drug use or disability. Rather it maintains that many of the problems people face are caused and/or maintained by social pressures. The argument is that my problems aren’t caused by the fact that I have no legs or that I hear voices but rather by the fact that society is organised in such a way that people with no legs cannot use services or that voice-hearers are stigmatised.
A good example might be the London underground service (the tube). Originally the vast majority of tube stations were accessible only by stairs which, of course, meant that wheelchair users couldn’t access the platforms and so couldn’t use the tube. Is this problem caused by their disability or is it caused by the fact that society ignores the needs of many citizens?
The social model argues that society has a responsibility to all – not just to those with a particular set of attributes. It is because of social model concerns that so many tube (and other) stations have now been fitted with mechanical lifts large enough to accommodate wheelchairs. It’s a social solution to a problem that arguably needn’t be thought of as ‘medical’ at all. People may well have physical differences but the real impact of those problems is caused by the way that society responds to them. This is why we have laws governing discrimination and ensuring fair access to services and employment.
In terms of mental health and disorder (the real focus of this blog) the social model argues that the way society responds to people who are psychologically different is the real problem. The social stigma surrounding mental disorders can be an effective barrier to inclusion, employment, insurance, housing and many other aspects of our society that other people take for granted. The effect of such exclusion and alienation on self-esteem and life opportunities is well known to be extremely detrimental.
There’s an interesting (and relatively recent) illustration of the difference between the social model and the biological (medical) model that we discussed earlier. Until recently homosexuality was thought to be a mental disorder. This took all responsibility away from the larger society and so if gay men and lesbians were unhappy that was thought to be a function of their disorder. Today in UK society most people see homosexuality as no more than an individual trait. It’s not illness – it’s just a part of a person’s larger identity. Social stigma has reduced dramatically and presumably will disappear almost completely within another generation or so.
By taking homosexuality out of the medical model and placing it within a social context many (although admittedly not all) problems with discrimination have been solved by social attitudes changes. Now if someone is depressed and also happens to be homosexual we deal with their depression without sticking medical labels upon their sexuality.
A large part of the change we have seen in recent decades has been due to the influence of the ‘gay pride’ movement and there is a direct similarity between the way that gay and lesbian people previously were seen in our society and the suspicion that surrounds people diagnosed with mental disorders today. Because of this the ‘mad pride’ movement has taken some very direct lessons from the gay movement and mad pride events are becoming increasingly common in Britain today.
It will be interesting to see what happens to the stigma around people who hear voices or who believe that they can commune with unseen entities over the next few decades. After all if it’s OK for priests, pastors and faith healers to hear and talk to their Gods, angels and guides and it’s acceptable for mediums to commune with the ‘spirits’, why should it be any different for people who believe that they can talk to the Martians?
Perhaps the only real difference between the priest, the madman, the shamanic healer and the medium is social acceptance.
Merging the two
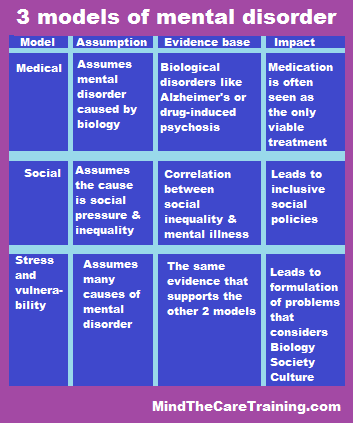
So far we’ve looked at two basic models that seek to explain mental health and disorder. We considered the medical model that places the root of disorder in the physical body and the social model that identifies social problems as the root cause.
Both these models have their advantages but neither is sufficient on it’s own. What we really need is a way to think about (and deal with) mental health problems that acknowledges more than just a single cause. The possibility of a genetic or chemical characteristic in people diagnosed with certain mental disorders doesn’t mean that there are no other factors to be considered as well. Similairly, social drift or other such problems don’t remove the possibility of biological issues. Both the social and medical models are limited (at least in their pure forms) because both exclude the knowledge and understandings of the other.
The ‘stress and vulnerability’ model encompasses both these paradigms and more. Beginning with the basic premise that distress results from stress we concern ourselves with the various types of stressor that create problems and also the different factors affecting vulnerability. Some people are more vulnerable to stress (or particular types of stress) than others.
There are five basic types of stressor. One of these is ‘biological’ which corresponds to the medical model. The social model is covered by two others – the ‘social’ and ‘cultural’ stressors. Additionally the model includes ‘psychological’ stressors and ‘developmental’ stressors. Developmental stressors can variously be seen as biological or socio-cultural as well depending upon the exact nature of the stressor. Put simply then the five stressor types are:
- Biological;
- Social;
- Cultural;
- Psychological;
- Developmental.
Some people are very susceptible to stress whereas others are not (although even the strongest among us has limits). Not only that but different people have different types of susceptibility. One person may be very susceptible to psychological stress but biologically robust whereas another might be quite the opposite. This degree of susceptibility to stressors is what we mean by vulnerability.
So according to the ‘stress and vulnerability’ model distress or disorder is what happens when the stress we face is greater than we can cope with. Let’s look at a few simple examples….
The biological stressor of drug misuse can tip biologically vulnerable people into mental disorder of various kinds whereas others who are less vulnerable to biological stressors may be unaffected.
A person with marked social vulnerability might develop problems after rejection whereas another, less gregarious individual might take it in their stride.
A person with a strong ‘internal locus’ of self esteem might take criticism with a pinch of salt but find themselves extremely vulnerable to psychological stressors such as self reproach or guilt.
Some people are so vulnerable to a range of stressors that they seem to be distressed or mentally disordered ‘all the time’. Traditional psychiatry has assumed that this must be because they simply ‘are’ mentally ill people whereas the social model holds that they are constantly treated unfairly by others. Stress and vulnerability holds that they need help to deal with their stressors across any or all of the five groups.
This leaves us with two basic tasks.
- Work on reducing stress levels and help the individual to learn how to manage their own stressors;
- Help people to reduce their vulnerabilities across any or all of the five basic types of stressor.
Recovery happens when a person’s stress reduces, their coping ability increases or both to the extent that they can handle life without becoming more disordered than the average person.
To arrange training for your staff please complete the contact form below…


I really struggle to see how the stress and vulnerability model work for serious mental illnesses. Schizophrenia appears out of the blue at typically a relatively young age,and while you can always pick through anyone’s life and find stressors to suggest that the problem is stress seems completely out of proportion. It’s certainly true that a stress free life helps people manage as life goes on, it just doesn’t seem to fit with the reality of schizophrenis
LikeLike
Hi Judy B,
Thanks for commenting.
The model uses the word ‘stress’ in a slightly different way from lay society. There are 5 different types of stress including biological (organic physiology, substances, physical illness, sleep disorder etc) which many might argue are the most important factors in disorders like schizophrenia. Even so the impact of other stresses on individuals with diagnosed disorders like schizophrenia is also important. It’s remarkable how much difference can be made on a person’s quality of life and functioning by changing environment and social factors, for example.
LikeLike
Reblogged this on Perfectlyfadeddelusions.
LikeLike